Abstract
Dental composite materials continue to improve, and using the latest curing technology can further unlock their potential.
Learning Objectives
- Gain an understanding of the benefits and drawbacks of bulk fill dental composites
- Discover how curing laser technology works and the efficiencies it can add to restorative dental procedures
I remember going to get some lumber with my grandfather in his pickup truck. I lived in Kansas City, Missouri, and the city sits on the corner where the Missouri River makes a hard turn east and heads toward St Louis. My grandfather and I were headed for a lumberyard on the north side of the river.
The night before there had been a huge rainstorm that had dumped a record-setting amount of rainfall on the area. As we were crossing the bridge over the Missouri River, I looked out the window of the truck and noted to my grandfather, “Wow! It looks like the water is almost up to the bridge!”
My grandfather always enjoyed mixing in philosophy when educating me and I will always remember him smiling at me and saying, “Sometimes you don’t raise the bridge, you lower the river.”
Bewildered, I asked, “What does that mean?”
He smiled slyly and said, “It doesn’t make much sense now, but it will later. Trust me.”
My grandfather’s education stopped when he completed the sixth grade in a 1-room schoolhouse, but in a lot of ways he was smarter than many people I know who have postgraduate degrees. Over the years, his old-school philosophy has helped me to better understand the world as well as to help me make much better decisions.
Lowering the River in Adhesive Dentistry
I know some of you are now wondering what the heck my grandfather’s philosophy has to do with dental composites…. But hear me out.
We follow guidelines to ensure success. Some of these guidelines are for safety or other truly critical reasons, and some are things you must do because of the limitations of tools or materials.
For example, materials used to fabricate dental crowns have minimum reduction limits to allow for adequate bulk of material. This is the minimum amount of material that can exhibit the expected physical properties. Making a lithium disilicate crown too thin will doom it to fracture. We aren’t prepping a tooth because we want to remove more tooth structure than necessary; we are preparing enough room around the tooth to allow the restorative material to have adequate strength and therefore fracture resistance.
So let’s apply this to direct composite restorations. For years we have been taught the philosophy and technique of incremental placement. The concept has 2 basic tenets. The first is that as they polymerize, composites shrink and occupy less physical space. The second is that curing lights must reach the entire increment that has been placed.
The reason that we follow these 2 rules? Simply put, it is because they were necessary at the time they were created. Now we are doing so because we were taught that way mixed with “Because we’ve always done it that way.”
Early composites would shrink quite a bit as they cured, so the idea of incremental placement had the doctor place small amounts, usually in 2- to 3-mm increments so the stress created by shrinkage during curing was applied to each individual increment, spreading out and thus minimizing its impact. Each increment—due to its size and the physical properties of the composite material—shrank when cured. Then another increment was placed over this previously cured material. The idea was sound because this spread the polymerization shrinkage over multiple layers, which decreased the overall stress on the tooth being restored.
However, as composites have evolved, their polymerization shrinkage has decreased. Current materials do not shrink as much as previous generations. This has brought about the concept of bulk fill composites that are placed in a single increment. However, the one problem with light-cured, bulk fill composites is effective photopolymerization.
In addition to early-generation dental composites exhibiting greater polymerization shrinkage, clinicians were also limited by the available curing light technology. To properly reach the material and completely pass through it from top to bottom, a curing light had to deliver a certain amount of energy. If, for any reason, the energy delivered was inadequate, the material would not cure properly, which would result in postoperative sensitivity, material breakdown, and the ultimate failure of the restoration.
The practice of incremental placement helped with the curing light power problem as well as the material shrinkage problem. Not only did small increments decrease shrinkage stresses, but they also allowed lower-powered curing lights to get photons through these increments from the top to the bottom. This helped create restorations that were cured as well as possible considering the limitations of the hardware.
Turn It Up
Catapult Education, LLC is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry.
Approved PACE Program Provider. FAGD/MAGD Credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. 6/1/20 to 5/31/24. Provider ID 306446.
Catapult Education designates this continuing education activity for 1/4 credit.
Sponsored by:
Online Quiz
For more info on this activity, or to take the quiz and obtain your continuing education credit follow the link from the QR code or visit www.catapulteducation.com/course/laser-curing
Science never stands still and as research and development continued, smaller and, more importantly, higher-powered curing lights were brought to market. These lights provided the ability to cure increments in shorter periods.
Bulk fill materials also were brought to market. To compensate for the limitations of curing light technology, the materials were more translucent than other dental composites. This allowed photons to penetrate further into the material to allow for bulk curing, but the esthetics of the materials were lacking. It saved time, but in the give-and-take of using early bulk fill composite materials, those time savings came at the cost of a less esthetic restoration.
Many doctors appreciated the efficiency bulk fill composites brought to restorative procedures, but the translucency caused the materials to appear a bit gray.
There was also the problem brought about by curing these deeper layers of composite. Every curing light on the market has a maximum output that depends on the manufacturer’s design. That means that one light might provide greater depth of cure than another. This caused confusion in offices with different brands of curing lights, and it made troubleshooting more difficult on those occasions when sensitivity occurred. What dentistry needed was a predictable depth of cure.
However, confidence in the depth of cure must be balanced with the need for efficiency. Any time a doctor starts the process of placing a composite restoration, a game of “beat the clock” commences. Adhesive dentistry is sensitive to technique, and the longer the process takes, the greater the chance of the restoration process being derailed due to contamination from blood, saliva, or crevicular fluid. Short curing times make the process easier, faster, and more predictable. Neither the patient nor the doctor wants appointments to take longer, especially the doctor who knows that any type of contamination increases the possibility of postoperative complications.
Follow the Light
Although the physical properties of dental materials continue to improve with reduced polymerization shrinkage and deeper depths of cure, it is also important to consider advancements in technologies for the polymerization process. Since their introduction, LED curing lights have been the standard technology for intraoral curing of dental materials because of their broad-spectrum light output, high intensity, and minimal heat generation.
However, there is now a more powerful curing option in the form of solutions such as the Monet Laser Curing Light from CAO Group.
A curing laser offers several unique advantages over traditional LED curing devices. A curing laser can produce more than 2 to 3 times the energy output of an LED curing light. A laser produces approximately 2400 to 4500 mW/cm2 of power compared with most LED units on the market that produce roughly 1300 mW/cm2 of output at regular power with some reaching approximately 3000 mW/cm2 with Boost Mode settings.
With the higher-intensity laser light, clinicians can cure material in less time than with an LED light. An LED curing light might have curing cycles of 10 or even 20 seconds, but a laser curing cycle can be as short as 1 second. A sometimes overlooked benefit of these short curing cycles is also they greatly decrease the chances of contaminating the field.
By their nature, lasers are coherent beams of light, that makes it easier to collimate the beam so the stream of photons does not diverge as it exits the head of the light. This keeps the photons concentrated on the target tooth/restoration while also providing uniform and predictable intensity. Most LED curing lights provide a divergent beam that sprays the photons in a wide area, and many do not have the full intended impact on the photopolymerization of the composite material. Instead, the beam disperses the farther it gets from the light source. As those photons spread out the power of the beam is reduced and more of the light strikes the surrounding tissue and has no effect at all.
Collimation also means there is very little decrease in intensity drop-off due to distance.It is always advisable to get the curing device as close as possible to the target. However, this is difficult, if not impossible, to achieve when curing a proximal box or a deep area on the floor of any prep. Reaching those hard-to-reach places with a curing laser is much more reliable because of its collimation. It also provides a more reliable depth of cure.
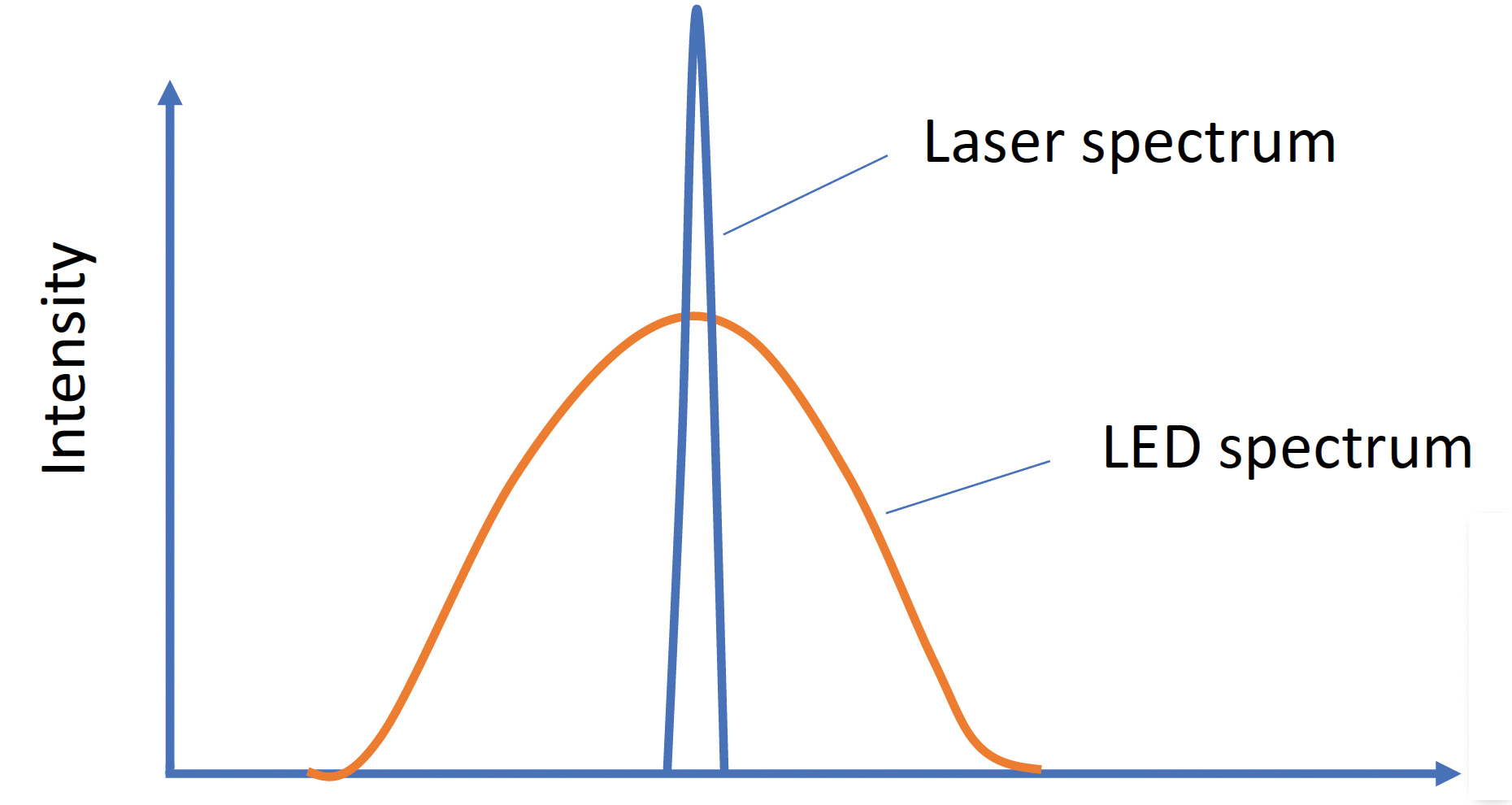
Lasers are also monochromatic, which means the photons are all of 1 specific wavelength. This means the photoinitiator’s absorption at that wavelength is maximized (Figure 1).
The intensity of the beam and its collimation translate to an impressive depth of cure. As I mentioned earlier, one of the reasons for incremental curing was that small increments allowed the curing light photons to reach the bottom of the material increment. Laser curing technology provides greater depth of cure with significantly less time.
Wrapping Up
Curing is incredibly intrinsic to the clinical success of adhesive restorations, whether they are direct composites or indirect bonded prosthetics. High-intensity cures that provide better depth of cure in less time are now a reality. These amazing results are attainable by using a handheld curing laser.
Just like my grandfather pointed out at the bridge, sometimes to get to a new solution, you have to look at the problem from a different vantage point. If you want to up your game when it comes to bonded restorations, consider adding a curing laser to your armamentarium.